FRN Research Report July 2015: Remission Rates Provide Better Outcome Measures for Substance Use Disorder Treatments
Background
Addiction treatment is a paradoxical issue in the United States. While the majority of medical and scientific institutions define addiction as a chronic disorder, too often it is treated on an acute basis. Expecting addiction to respond to a single, acute-style treatment is unrealistic: as a chronic disease, addiction requires a continuum of care. Additionally, measuring the impact of treatment using an acute definition, such as cured, is also inappropriate. A better evaluation of addiction treatment measures how long a person stays symptom-free, or in remission.
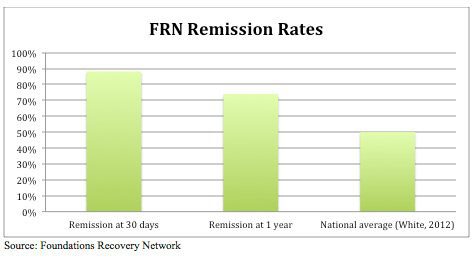
Although popular opinion on the long-term benefits of addiction treatment varies, patients who follow evidence-based protocols can achieve remission. Remission is defined as the absence of symptoms. This differs from abstinence because it is not a measure of substance or alcohol use, but instead a medical indicator of the presence of a disorder or disease based on the industry standard diagnostic criteria found in the Diagnostic and Statistical Manual of Mental Disorders. In fact, the overall remission rate for a substance use disorder is similar to remission rates for other chronic diseases, including cancer, diabetes and asthma (McLellan, Lewis, O’Brien, & Kleber, 2000). Substance use disorder (SUD) remission rates for patients treated at Foundations Recovery Network (FRN) facilities are much higher than the national average (based on White, 2012), revealing the benefits of FRN’s ongoing support programs.
FRN centers offer a broad range of evidence-based services that include Motivational Interviewing, Cognitive Behavioral Therapy and Dialectical Behavior Therapy skills, as well as specialized therapies for trauma and co-occurring disorders. While evidence-based addiction treatments are not consistently available across the United States, they are the recommended standard for all facilities. Some facilities offer treatments based on traditional or personal philosophy instead of scientific evidence, while other facilities have limited resources and do not offer a full range of services (Dennis & Scott, 2007). Foundations Recovery Network, with twelve integrated treatment centers, offers a nationally recognized system of care with research-proven methods.
Patients who enter treatment at FRN’s residential centers are offered the opportunity to participate in an ongoing study. Participants must sign Institutional Review Board approved consent prior to participation, and the follow-up study includes interviews at intake and again at 30 days, six months and one-year post-discharge. Data is collected using validated instruments, including the Addiction Severity Index and Treatment Service Review as well as items from Quality of Life scales and depression and anxiety assessments. Included in the interview are the DSM criteria for the presence of a substance use disorder. These questions are designed to determine whether the former FRN patient is in remission.
Remission Rates and Chronic Disease
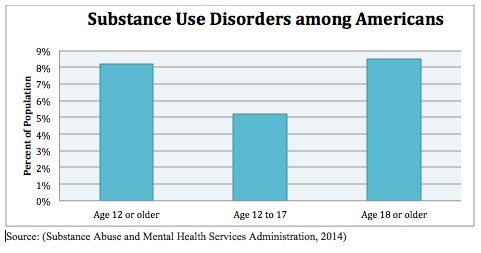
This paper focuses on the importance of using remission rates as a measure for evaluating a person’s response to treatment. Addiction affects an estimated 21.6 million Americans, but only a small percentage of the people who need treatment (2.5 million) get it at a specialty facility (Substance Abuse and Mental Health Services Administration, 2014). Some people forgo professional treatment because they believe it isn’t effective. This belief comes from a traditional acute care approach to addiction that expects a single period of treatment to cure the disease. In addition to discouraging people from seeking treatment, this idea limits the resources lawmakers allocate to the disease, and it influences health insurance policies (Dennis & Scott, 2007).
American institutions recognize the chronic nature of addiction, but there is still widespread misunderstanding about the effectiveness of addiction treatment (American Psychiatric Association, 2000) (American Society of Addiction Medicine Board of Directors, 2011) (National Institute on Drug Abuse, 2005). Too often, addiction treatment is evaluated by short-term outcomes. Observations over brief periods do not fully capture a person’s success over a lifetime. Plus, the practice of judging a person’s symptoms on a single episode of treatment makes it easier to assume poor outcomes. Evaluating a person’s symptoms over a longer period, such as several years, makes recovery an expected outcome (Institute for Behavior and Health Addiction Treatment Outcomes Working Group, 2014).
While abstinence rates show how long a person goes without taking a substance, remission rates show a more detailed picture of progress. Remission is the symptom-free stage of a chronic disease. Physical illnesses, such as cancer, diabetes and asthma, are treated actively to reduce symptoms and then treated through ongoing maintenance therapies to monitor the return of symptoms (White & McLellan, 2008). Since chronic diseases have no cure, the success of treating these diseases is measured by remission rates (McLellan, Lewis, O’Brien, & Kleber, 2000).
All chronic diseases require more complex treatments than acute disorders, such as a bacterial disease or a broken bone. While an acute condition can be cured through a basic treatment plan, a chronic condition is affected by biological, psychological and social factors. Treating any chronic condition requires three steps. In the first stage, treatment can reduce or eliminate symptoms but still not cure the initial cause of the disease. The second stage begins once symptoms are managed; patients must make lifestyle and behavior changes to maintain control of symptoms. The third stage is the most complex part of the process. A person needs ongoing monitoring and support to stay in remission. A minor lapse or even full relapse is common after initial treatment because of the intricate steps required to control symptoms (White & McLellan, 2008).
Defining Remission for Substance Use Disorders
The Diagnostic and Statistical Manual of Mental Disorders, the US standard for defining mental disorders, outlines the clinical stages of remission for SUD. Generally a person is in remission when she no longer exhibits signs of dependence or substance abuse. Dependence is the more severe form of SUD; a person qualifies for substance abuse when she experiences only a few symptoms of the disorder (Substance Abuse and Mental Health Services Administration, 2004). The DSM outlines the major symptoms of substance dependence. When a person is free of all of the symptoms (excluding craving), she is in remission.
Psychological symptoms affect a person’s ability to control substance use. A person may take more of a drug than intended or take it over a longer period. She also may fail at attempts to stop taking the drug or cut down on the amount of the drug. She will also spend more and more time on activities associated with the substance, such as visiting multiple doctors or chain-smoking. Quality of life is damaged as the person avoids important social, occupational or recreational activities due to substance use. Dependence also includes a person’s continued use even when she knows the substance causes physical or psychological problems.
On average, there are an estimated 25 million to 40 million people in the United States in remission from SUDs, or around 5.3% to 15.3%. Of the people who once met lifetime criteria for SUDs, an average of 49.9% no longer meet the criteria (White W. L., 2012).
Remission rates at FRN facilities are much higher than the national average. Around 88% of patients met the qualifications for early remission at 30 days post treatment, and nearly 74% met the qualifications for remission at one year.
FRN maintains scientifically sound research models, and an independent third party verifies research results. Enrollment in its research programs and corresponding response rates exceed federal minimum standards, supporting the validity of findings. SAMHSA requires 80% of patients to enroll in programs and 60% of them to respond in order for data to be considered reliable. Consistently for the past three years, FRN has achieved a 90% or better enrollment rate. Currently, overall response rate averages at 72% (June 2015 FRN management report).
FRN’s high patient participation rates reflect strong engagement in treatment programs. Patients who are invested in the treatment process are more likely to have better outcomes. Furthermore, patients who believe in the long-term success rates of addiction treatment have a higher rate of maintaining remission. Research on personal attitudes about relapse show a connection between beliefs about the disease and success with long-term coping skills (Marlatt & Donovan, 2005).
Conclusion
While the medical community considers addiction a chronic disease, treatment outcomes are often viewed through an acute care lens. A side effect of this approach is the belief that addiction may be cured at the end of the treatment stay (White & McLellan, 2008). Furthermore, older ideas that addiction is a moral problem or an indication of weak character has led people to believe that willpower is a valid cure (White W. L., 2012). Understanding the clinical reasons behind addiction and measuring outcomes against medical criteria makes better treatment possible. Ideas that addiction is a moral issue or can be “cured” with willpower hamper people from seeking treatment, lower government funding for treatment programs and research, and criminalize people who are suffering from the disease (Broadus & Evans, 2015).
Foundations Recovery Network is committed to research that improves treatment for all addicted individuals. If you would like to speak with an admissions coordinator today or if you would like to learn more about our research methods and programs, please call us directly at 615-490-9376.
References
American Psychiatric Association. (2000). Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR). Washington, DC: American Psychiatric Association.
American Society of Addiction Medicine Board of Directors. (2011, April 19). Definition of addiction. Retrieved July 10, 2015, from American Society of Addiction Medicine.
Broadus, A. D., & Evans, W. P. (2015). Developing the public attitudes about addiction instrument. Addiction Research & Theory, 23(2), 115-130.
Dennis, M., & Scott, C. K. (2007). Managing addiction as a chronic condition. Addiction Science & Clinical Practice, 4(1), 45-55.
Institute for Behavior and Health Addiction Treatment Outcomes Working Group. (2014). Creating a new standard for addiction treatment outcomes. Institute for Behavior and Health. Rockville, MD.: A Report of the Institute for Behavior and Health.
Marlatt, G. A., & Donovan, D. M. (Eds.). (2005). Relapse prevention: Maintenance strategies in the treatment of addictive behaviors. New York, NY: Guilford Press.
McLellan, A. T., Lewis, D. C., O’Brien, C. P., & Kleber, H. D. (2000). Drug dependence, a chronic medical illness: Implications for treatment, insurance, and outcomes evaluation. The Journal of the American Medical Association, 284(13), 1689-1695.
National Institute on Drug Abuse. (2005, June). Addiction is a chronic disease. Retrieved July 10, 2015, from National Institute on Drug Abuse.
Substance Abuse and Mental Health Services Administration. (2004). Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction. In (Treatment Improvement Protocol (TIP) Series, No. 40.) Appendix C DSM‐IV‐TR Material.. Rockville, MD: SAMHSA.
Substance Abuse and Mental Health Services Administration. (2014). The NSDUH Report: Substance Use and Mental Health Estimates from the 2013 National Survey on Drug Use and Health: Overview of Findings. Center for Behavioral Health Statistics and Quality. Rockville: SAMHSA.
White, W. L. (2012). Recovery/Remission from Substance Use Disorders: An Analysis of Reported Outcomes in 415 Scientific Reports, 1868-2011. Philadelphia: Philadelphia Department of Behavioral Health and Intellectual disAbility Services and the Great Lakes Addiction Technology Transfer Center.
White, W. L., & McLellan, A. T. (2008). Addiction as a chronic disease: Key messages for clients, families and referral sources. Counselor, 9 (3), 24-33.