FRN 2017 Results: Our Methods, Principles Practices, and Results
Key Differentiators
Our Effectiveness: Research and Outcomes
At Foundations Recovery Network (FRN), we follow patients using research-based interviews for a full year after treatment. Patients are contacted at 30 days, six months and one year post- discharge. This allows us to determine not only the immediate impact of treatment, but also the sustainability of results. In 2017, 88% of patients enrolled in our outcomes research program and 65% of patients were reached for follow-up surveys.

Past 30 day use is an indicator of current use. The Substance Abuse and Mental Health Services Administration (SAMHSA) collects and reports past 30 day use in the National Survey on Drug Use and Health (NSDUH) annually as a measure of the magnitude of substance use. Patients entering treatment at FRN facilities used alcohol for an average of 14.4 days during the 30 days prior to admission. They also reported drinking to intoxication 12 days over the prior month, using illegal drugs for over two weeks of the prior month (15.3 days) and using multiple substances an average of 10.7 days over the 30 days prior to admission. Patients also reported being troubled or bothered by psychological symptoms for an average of nearly three weeks (19.5 days) out of the prior month.
At one year post-discharge, patients were again asked about their use and symptoms over the prior months. Patients report an average reduction of over 12 days of alcohol use, including nearly 11 fewer days of intoxication on average. Similarly, patients used illegal drugs 13 fewer days and multiple substances nine fewer days one year after treatment. The average number of days of psychological symptoms was reduced from 19.5 to 4.7 days.
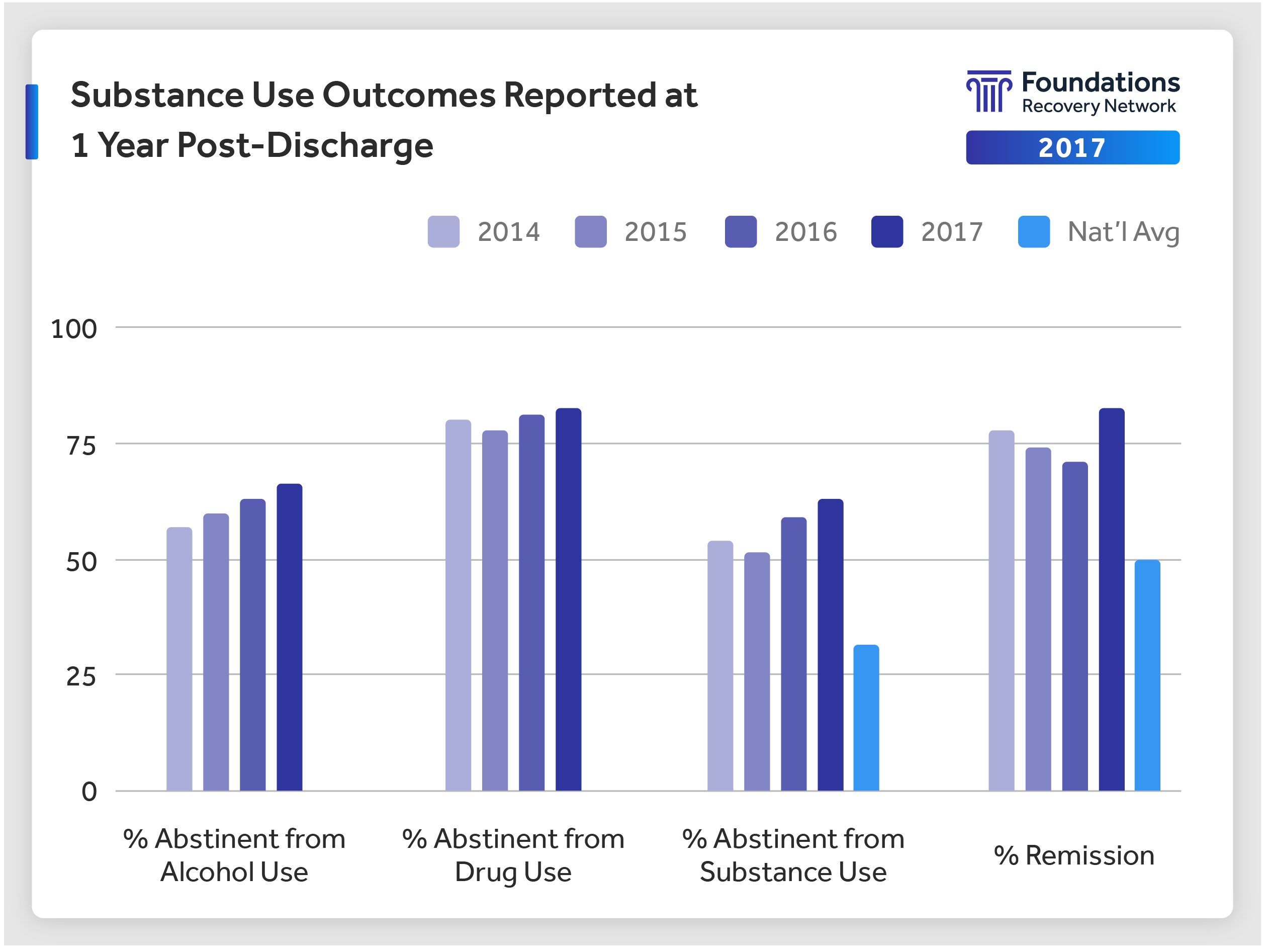
Substance use rates consistently compare favorably with the national average reported by White (2012). Remission rates represent the absence of clinical symptoms (excluding cravings) at the one year time point. Remission is determined based on the DSMIV-TR criteria used in diagnosing substance use disorders.
Substance abuse is often accompanied by mental health problems. At Foundations, we recognize that both disorders must be treated simultaneously and in an integrated manner. Mental health symptoms continue to improve or remain stable one year after discharge.
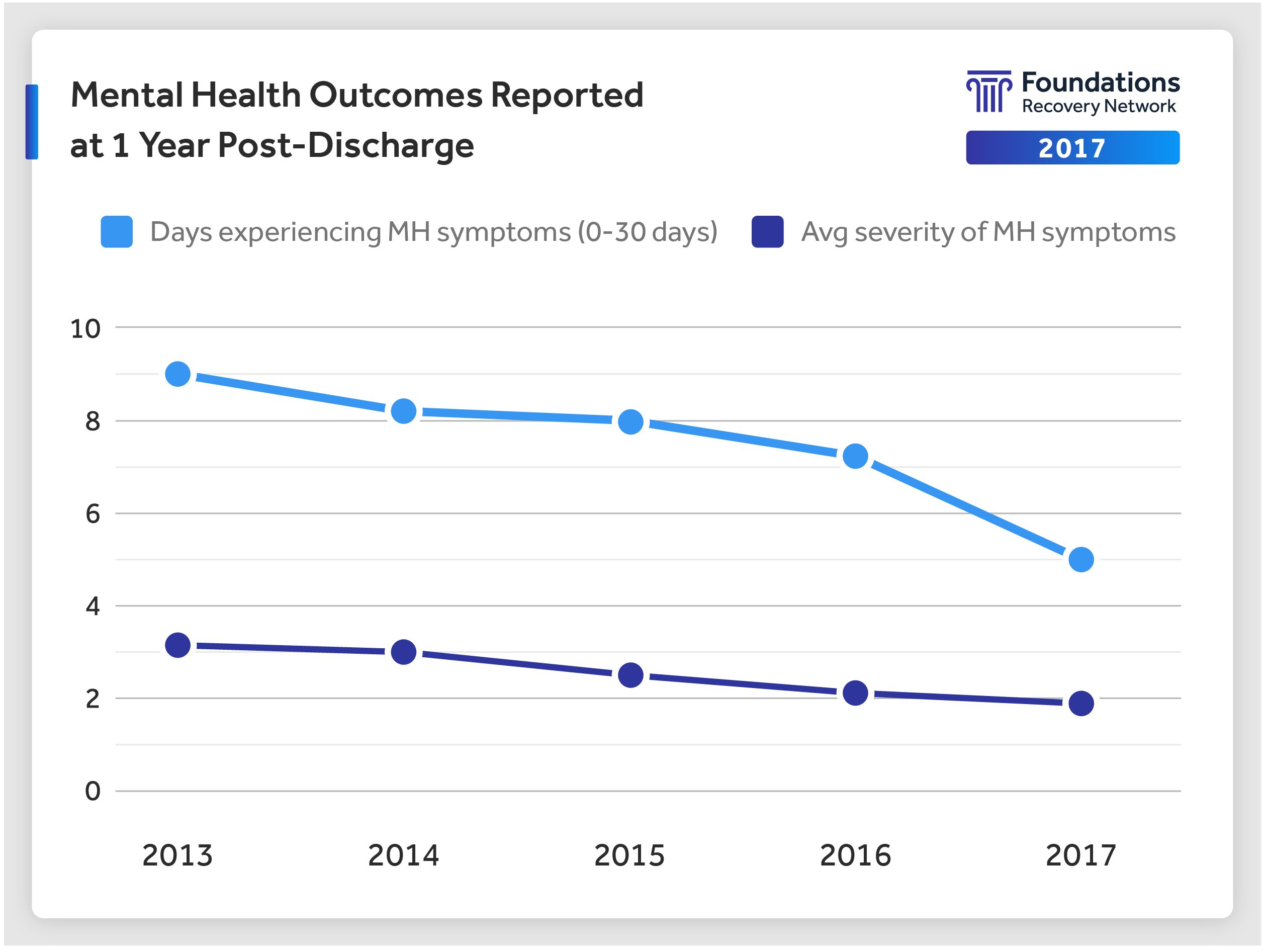
The above charts depict data collected over several years. Patients report significantly reduced days of symptoms as well as reduced severity of symptoms. Response rates vary by year with 65% of patients responding post-treatment survey in 2017. All years reported met SAMHSA standards for enrollment and response rates.
Our Fidelity: Excellence in Dual Diagnosis Treatment
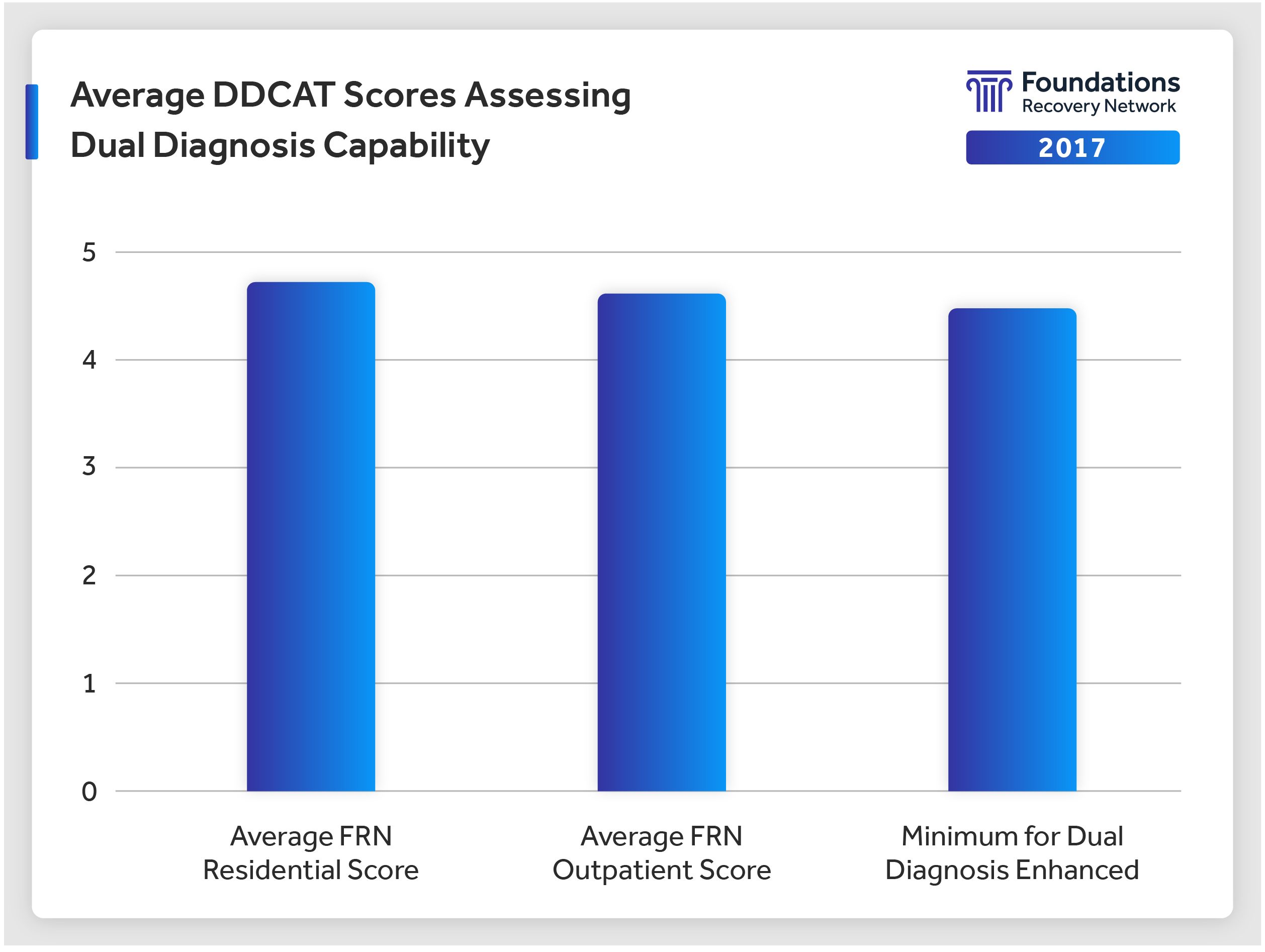
Foundations Recovery Network is a nationwide provider of integrated treatment for co-occurring addiction and mental health disorders. We offer dual diagnosis treatment across all of our programs, annually meeting criteria for “Dual Diagnosis Enhanced” (DDE) services, a standard only achieved by the top 5 percent of addiction treatment programs.
Eligibility for DDE services is determined by the Dual Diagnosis Capability in Addiction Treatment (DDCAT) index assessment. Dr. Mark McGovern, a member of Dartmouth Psychiatric Research Center and one of the developers of the DDCAT, classified FRN’s program as the “gold standard” in the treatment industry.
Our Patient-Centered Care: Satisfaction with Admission and Treatment Experience
Patient satisfaction is a key determinant of quality of care and strongly influenced by expectations of care and attitudes. Patient satisfaction is also associated with patient engagement in treatment: Higher levels of satisfaction with treatment support greater engagement, which, in turn, is a predictor of outcomes.

The willingness to recommend a service to others is a strong indicator of satisfaction with service. On average, 90 percent of patients surveyed at discharge from an FRN residential facility would recommend the treatment center they attended to others. Scores below represent the level of agreement or likelihood patients would recommend the treatment center they attended (scale=1-5).
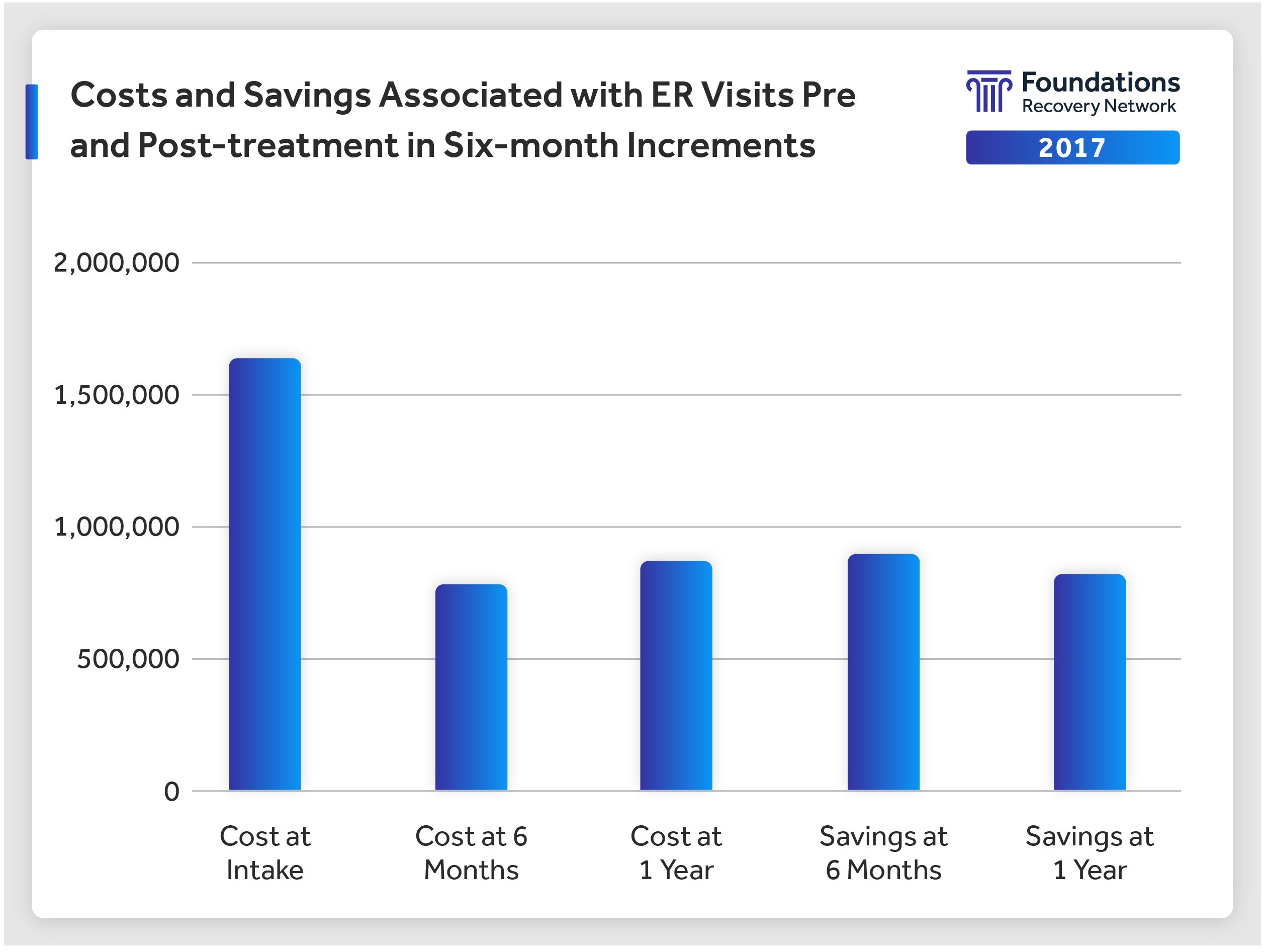
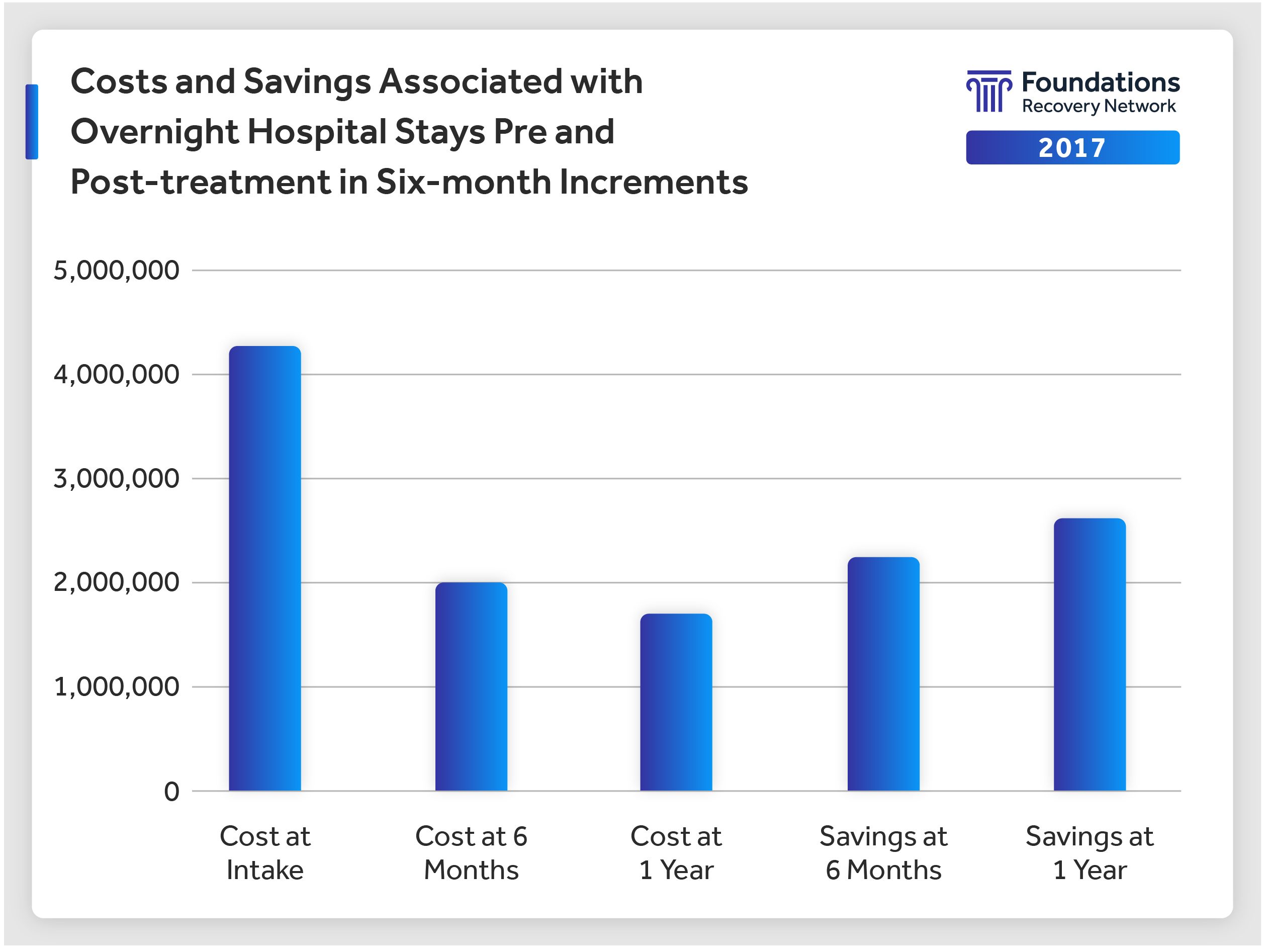
Our Savings: Estimated Changes in Healthcare Utilization for ER Visits and Hospital Admissions for All Causes
Foundations conducted an analysis of the ER visits and hospital admissions in 1,890 patients attending treatment. When compared to utilization in the six months prior to treatment, a nearly 50 percent reduction of costs was found for both the first and second six-month windows following treatment.
Use of emergency room services is one of the most costly entry methods into a healthcare system. In 2011, approximately 8 percent of the U.S. adult population had a substance use disorder and 18 percent had a mental health illness (SAMHSA, 2013).
Medical costs for treating patients with comorbid mental health/substance use disorder (MH/SUD) conditions can be two to three times as high as for those who don’t have these conditions. The National Council for Behavioral Health reports that the additional healthcare costs were estimated to be $293 billion in 2012 across commercially-insured, Medicaid, and Medicare beneficiaries in the United States (The National Council, 2015).
A large northern California managed care organization analyzed the medical costs incurred by patients who had attended treatment for substance use disorder. They found that there was a 35 percent reduction in inpatient costs and a 39 percent reduction in ER costs in those patients who attended treatment (Weisner, 2010).
Several studies also report significant healthcare cost differences in family members of persons with behavioral health disorders. Significant savings in family member costs were also found following treatment for the addicted family member (Ray, Mertens and Weisner, 2007).
Who We Serve
Understanding the demographics of our patient population is important. Research has demonstrated that certain demographic factors impact patient engagement. Patient engagement, or commitment and participation in treatment, is considered a strong predictor of long-term recovery outcomes with higher levels of engagement associated with positive outcomes (Choi, Adams, MacMaster and Seiters, 2013).
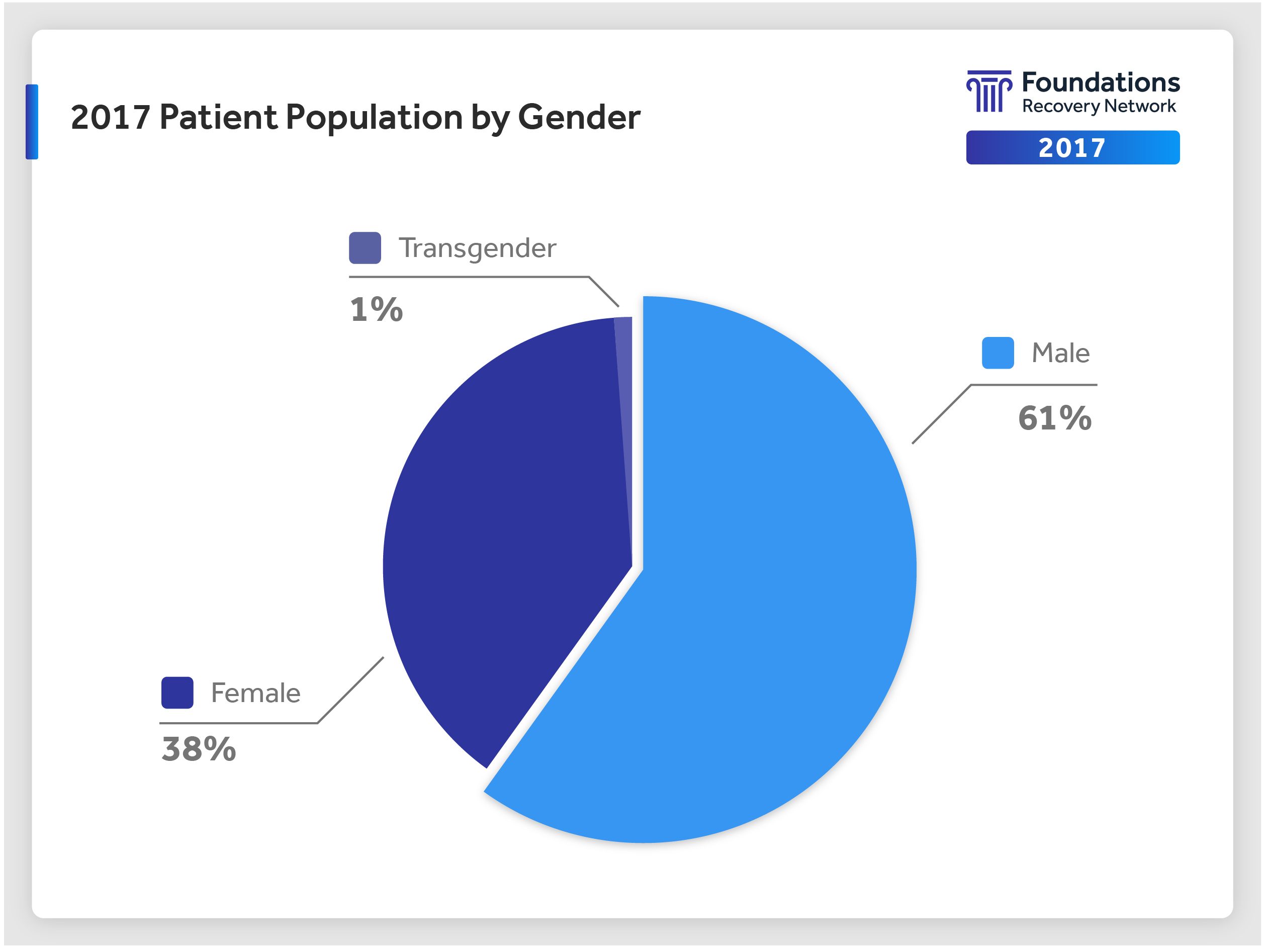
A majority of patients entering treatment at FRN facilities are male (61 percent). A small percentage are transgender (1 percent).
In 2017, the average patient age was 35; however, the most common age served was the young adult, with the modal age of our patient population at 24 years. Thirty-one percent of our patients were young adults (18-25), 37 percent were between 26 and 40 years of age, 25 percent were 40-55 years of age and the remainder (7 percent) were over 55 years of age.
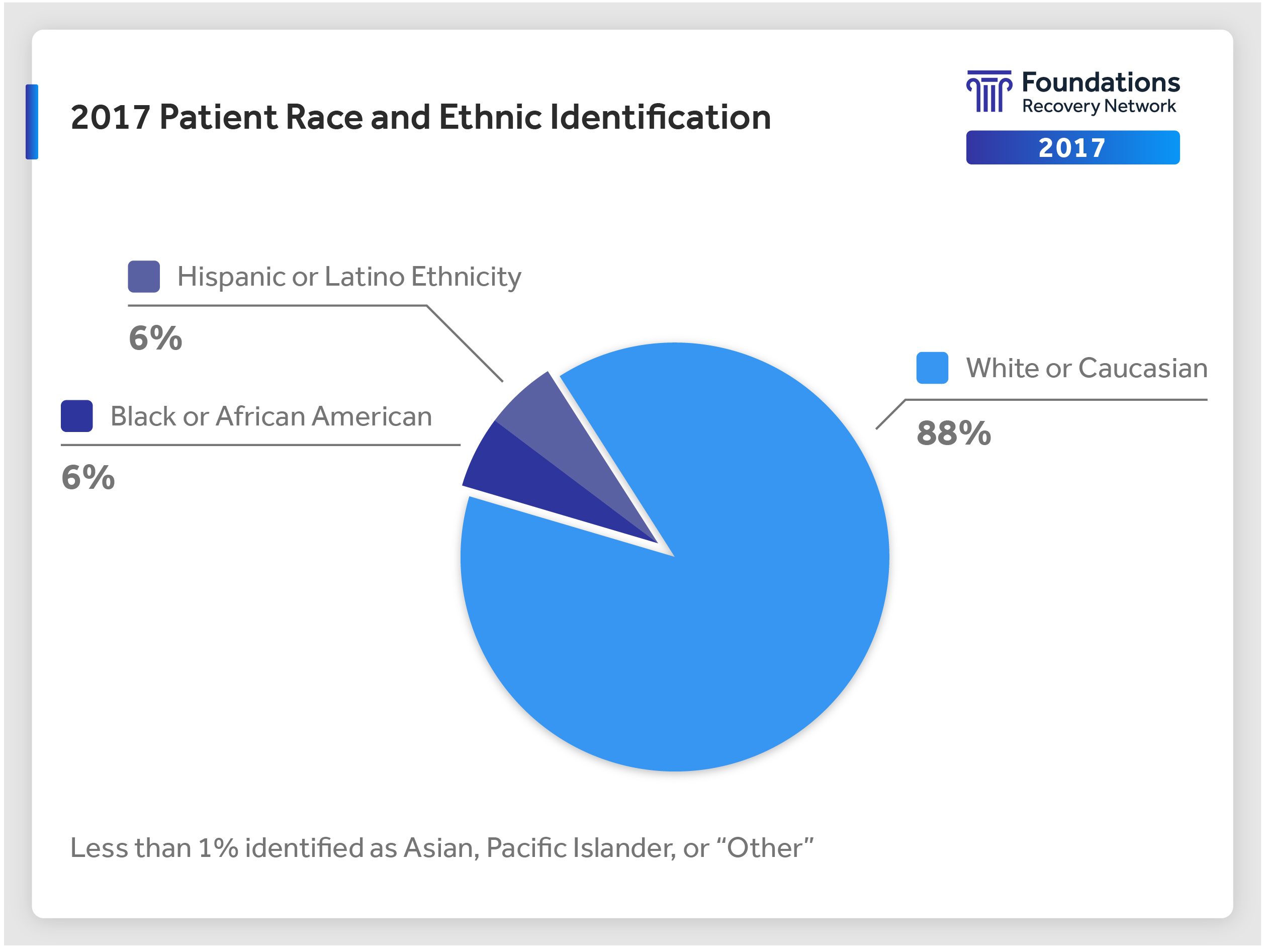
Additionally, our award-winning patient-centered care program integrates ethnicity and racial information into personalized treatment protocols. Most of our patient population identified as “white or Caucasian,” with 6 percent also identifying as “Hispanic or Latino.”
Understanding how patients self-identify with regard to gender and sexual preferences has led to the development of specialty tracks in some locations. About 12 percent of patients attending FRN facilities identify with the LGBTQI community, with a majority of those patients identifying as “gay” and a significant proportion who self-identified as “bisexual.”
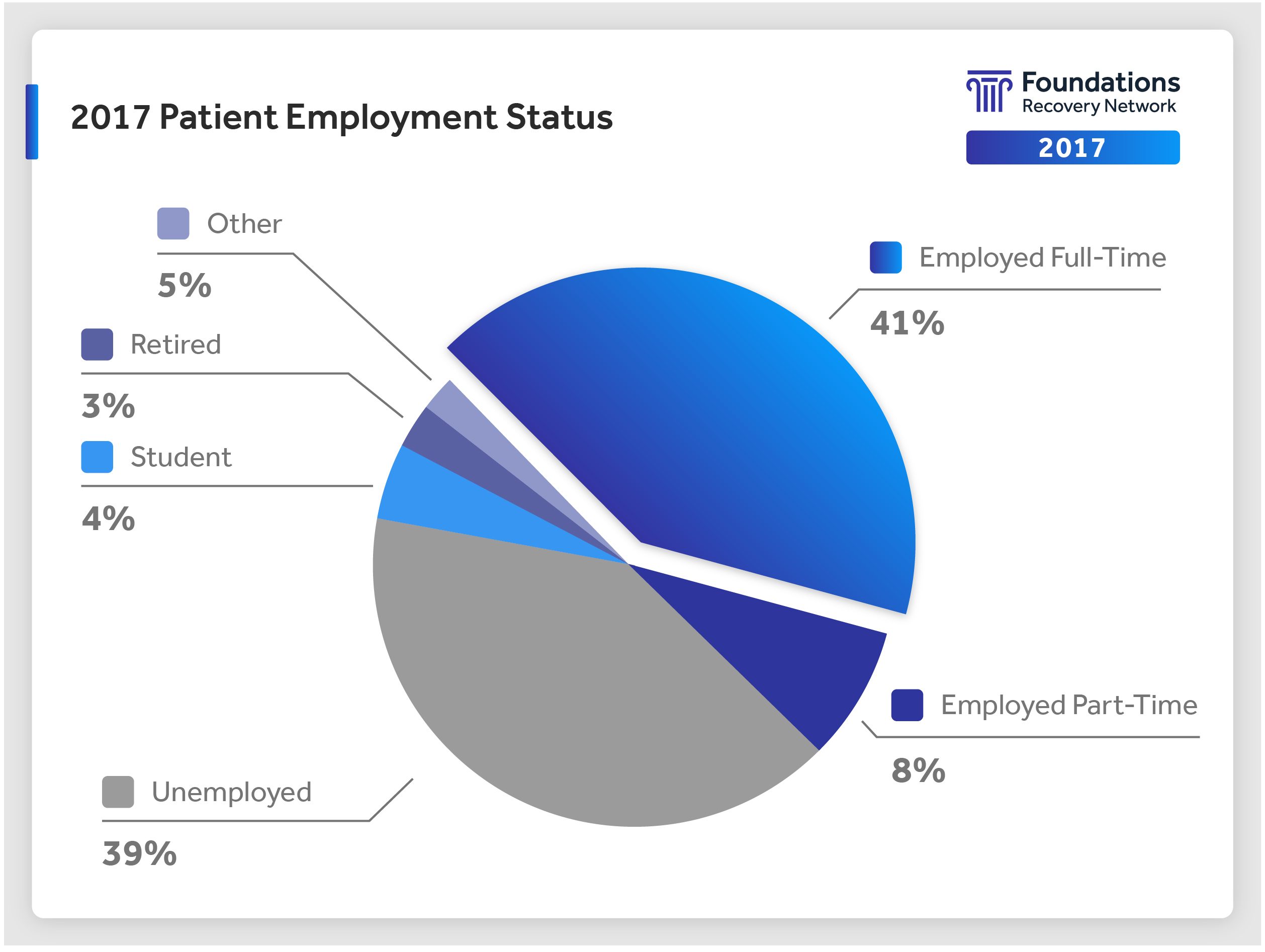
Employment status can have a significant impact on financial resources and a patient’s ability to remain in treatment for clinically recommended time periods. Patients who are employed or students may have to address outside issues while engaged in treatment. With seven residential facilities and 15 outpatient facilities around the country, our system of care meets patients where they are and supports them in engaging in appropriate treatment services, as well as meeting outside obligations in a therapeutic environment and transitioning to full and rewarding lives.
Our System of Care
The FRN System of Care is founded in our rich history as a national leader in dual diagnosis treatment. We value the history and tradition of our integrated system of care and further the philosophical foundation of this system with the introduction of a “no wrong door policy” within the program, which allows patients to seek support from all staff levels through cross-training and clear communication protocols.
The FRN System of Care was developed using federal guidelines for dual diagnosis treatment in SAMHSA Publication TIP 42, Dartmouth’s Dual Diagnosis Capability in Addiction Treatment (DDCAT) toolkit, evidence-based treatments such as the Stages of Change, Motivational Interviewing and Cognitive Behavioral Therapy, and through our research, outcomes and patient-centered care process.
Our Guiding Principles:
- Employ a recovery perspective
- Adopt a multi-problem viewpoint
- Address real-life issues
- Utilize a phased approach
- Plan for cognitive and functional impairments
- Use support systems to maintain and extend treatment effectiveness
Three of the main features underpinning the FRN recovery perspective are as follows:
- Recovery is a long-term process of internal change.
- Internal change proceeds through various stages (SAMHSA/CSAT 2005; DeLeon, 1996; Prochaska, 1992).
- Motivation is the key to change.
We have a core belief that everyone has the ability to recover and, therefore, we meet people where they are with acceptance and without judgment. Within this framework, FRN has outlined six guiding principles for treating dually diagnosed patients. These principles are reflected in the system of care at all process levels, from assessment through post-treatment planning.
The core components of FRN’s System of Care are the organizational expression of our philosophy and guiding principles. These core components integrate the most advanced practices in dual diagnosis treatment into our System of Care.
The FRN System of Care can be seen as a progression through levels of treatment. The System of Care is what makes FRN unique. It reflects our belief in the possibility of change and recovery for all. Through listening to our patients, we are able to provide a safe and healing environment with individualized treatment within the context of a structured program.
The continuity, functioning and comprehensiveness of the System of Care is supported through an integrated, modified community social model that embraces patient-centered care and supports staff development. We hold our programs accountable to the highest standards in integrated treatment and continue to evolve as new evidence suggests better methods of providing care.
Evidence-Based Treatment
Evidence-based treatments are based directly on scientific evidence. Most evidence-based treatments have been studied in several large-scale clinical trials, involving thousands of patients and careful comparison of the effects of evidence-based vs. other types of treatments. Dozens of multi-year studies have shown that treatments and practices that are evidence-based can reduce symptoms significantly for many years after discharge from treatment — similar evidence for other types of therapies (those not studied and determined to be evidence-based) is not available to date.
In practice, evidence-based treatment represents the marriage of “scientific evidence, clinical expertise, and individual patient needs and choices” (McKibbon, 1998).
An example of evidence-based treatment that makes a difference is the development of medication management skills (AHRQ, 2013). The average patient reports significant improvement in medication management, even one year following treatment. Additionally, fewer patients report missing medication doses following treatment at FRN facilities.